Heel pain - Plantar fasciitis
Anatomy
The basic anatomy of the plantar fascia is it originates from the medial tubercle of the calcaneus (heel bone) and inserts into the toes via tendons that flex the toes. There is a branch on the inside, a thick central branch and a branch on the outside. The central branch inserts into the base of all toes however the 1st also inserts into the sesamoid bones, this forms a bow like structure with the big toe joint
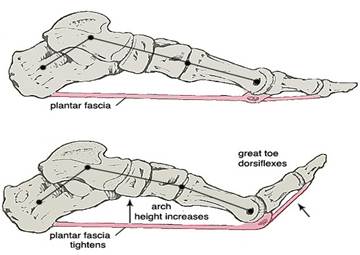
acting as a pulley. As a result when the big toe is pulled up the plantar fascia shortens and the arch rises.
Classic symptoms of plantar fasciitis include pain first thing on a morning or after a period of rest at the heel area and pain after prolonged weightbearing. The pain will be localised to the heel area, usually toward the inside and can be along the fascia itself.
It was believed that high tension in the fascia caused a bony spur to develop at the heel bone. However several authors question this as the spur is not always actually in or at the plantar fascia origin but located within other intrinsic musculature so this theory is now called into question.
There is much debate as to the term plantar fasciitis with authors finding a lack of inflammatory cells and evidence of degeneration should lead to the problem being plantar fasciosis instead. Despite this debate the treatment remains much the same.
Mechanics and Aetiology
When a force is placed beneath the big toe joint, when the arch is flattest or particularly high the plantar fascia tension is at its peak. Therefore if the force from the ground is high a high amount of force is required to flex the big toe joint into the ground to allow the big toe to move upward and raise the arch which provides a stable platform to propel the body forward.
If the ground reaction force is higher than the muscles can overcome to flex the big toe joint then tension remains in the fascia and the arch can not rise. This tension also causes the big toe to remain stiff and a resultant inefficient propulsive phase of walking. This repeated over a period of time with continued tension remaining in the plantar fascia is a likely mechanism for the injury.
A further factor is that as we age the elasticity of the fascia reduces therefore strain that we could have previously dealt with can become symptomatic. There may also be a role for compression force contributing to symptoms.
In autoimmune disorders plantar heel pain can present which is non mechanical in nature and will not respond well to treatments aimed at reducing strain in the fascia.
Treatment
Treatment should be aimed at reducing tension in the fascia. This can be achieved with an appropriate orthoses, appropriate stretching, taping, footwear changes and strengthening exercises.
Increased BMI, flatter or high arch foot types have been found to be risk factors for this condition as does having tight calf muscles.
Correct footwear is important in treating this problem (this includes indoors) with appropriate support. Often an appropriate footwear change can alleviate symptoms.
Debate in the literature continues as to the positive effect of steroid injections into the plantar fascia. There is some evidence to suggest that shock wave therapy can be beneficial.